

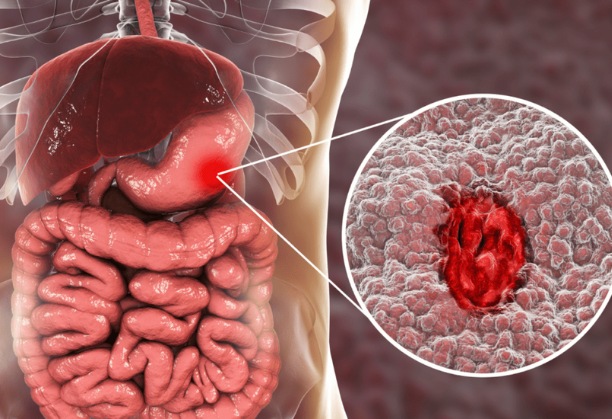
There are two prevalent types of peptic ulcer disease: those connected to the H. pylori bacteria and those connected to the consumption of aspirin and NSAIDs.
A Gram-negative, microaerophilic bacteria called Helicobacter pylori is primarily found in the gastric antrum of the human stomach. H. pylori is linked to 95 per cent or more of duodenal ulcers and 80 to 85 per cent of stomach ulcers.
H. pylori positivity increases the likelihood of peptic ulcer in long-term NSAID users, and it has been discovered that eradicating H. pylori in such individuals before starting NSAID therapy reduces the risk of H. pylori NSAID-associated peptic ulcer.
What is H.Pylori?
A Gram-negative rod bacteria known as Helicobacter pylori has lipopolysaccharides for cell adhesion and flagella for movement. The presence of urease enzymes on the surface of H. pylori, which convert urea and water into CO2 and ammonia, is one of the critical factors in the organism’s survival. Ammonia causes the stomach to become alkaline, allowing bacteria to use their flagella to migrate across mucus. After penetrating through the stomach’s mucus layer, the bacteria proceed to the columnar epithelial cells’ layer and adhere there using liposomes.
Pathophysiology
Production of cytotoxin-associated gene A (CagA) proteins, which cause cellular apoptosis and vacuolating cytotoxins, such as vac A, which trigger the inflammatory cascade by destroying the integrity of cells, are critical components of the pathophysiology of H. pylori infection. In addition, several H. pylori-produced enzymes, such as urease, haemolysins, neuraminidase, and fucosidase, may contribute to tissue injury. The primary hormone that stimulates stomach acid production is gastrin, and H. pylori infection also affects gastrin homeostasis. H. pylori-induced hypergastrinemia may be the cause of the duodenal ulcer’s hyperacidity.
Clinical manifestations
- Upper abdominal pain occurring 1–3h after meals
- Anorexia
- weight loss
- Nausea
- vomiting
- heartburn
Complications of peptic ulcer disease may occur with or without previous dyspeptic symptoms:
- Hemorrhage
- Chronic iron-deficiency anemia
- Pyloric stenosis and perforation
TREATMENT / MANAGEMENT
H. pylori cannot be eliminated by using antibiotics or acid-suppressing medications alone. Given that the organism’s growth occurs at a higher pH and antibiotic potency is increased during growth, both treatments work in concert.
A brief course of triple therapy with either
- omeprazole 20 mg, clarithromycin 500 mg, and amoxicillin 1 g or
- omeprazole 20 mg, clarithromycin 250 mg, and metronidazole 400 mg results in high eradication rates.
When coupled with metronidazole, a lower dose of clarithromycin (250 mg twice daily) is efficient and advised.
Treatment with a different triple therapy regimen will be necessary if a first-line regimen fails to eradicate the disease. A PPI, amoxicillin or tetracycline, and metronidazole are suggested second-line triple treatment regimens.
With a high prevalence of clarithromycin resistance, quadruple therapy may be employed as the first line of defense, which includes PPI, metronidazole, tetracycline, amoxicillin, and bismuth subsalicylate.